|
Intestinal anthrax in a 4-year-old
child
Professor M.H. Soltanzadeh MD
Professor of Pediatrics, ID ,
Shahid Beheshti University of Medical Science ,
Tehran ,IRAN
Siadati A MD1
,Shirvani F MD2 , Sardari M MD3 , Rashed F MD4
, Soltanzadeh M.H. MD , ID5 , , Shafagi B MD6
, Gharooni M MS7 | |
1- Ahmad Siadati MD ,
Professor of Pediatric Infectious Diseases , Markaztebi Hospital , Dr
Mohamad garib St. , Tehran University of Medical Sciences and Health
Services , (Tehran, Iran)
2 - Fariba Shirvani MD,
Assistant Professor of Pediatrics , Imam Hossein Hospital, Shaheed Madani
Street , Shaheed Beheshti University of Medical Sciences and Health
Services,(Tehran, Iran) Email:
shirvanif@yahoo.com
3 – Mehdi Sardari MD, General
Practitioner , Imam Hossein Hospital, Shaheed Madani Street , Shaheed
Beheshti University of Medical Sciences and Health Services ,(Tehran,
Iran)
4 – Farinaz Rashedmarandi MD,
Assistant professor of pathology, Director of department of microbiology,
Reference laboratory of Iran, research center, Boali Hospital, Imam
Hossein square, Damavand Street, (Tehran-Iran)
5 -Mohammed Hosein Soltanzadeh
MD , ID,Professor of Pediatrics , Imam Hossein Hospital, Shaheed Madani
Street , Shaheed Beheshti University of Medical Sciences and Health
Services,(Tehran, Iran)
6–Behroz Shafagi MD , Assistant
Professor of Pathology, Imam Hossein Hospital, Shaheed Madani Street ,
Shaheed Beheshti University of Medical Sciences and Health
Services,(Tehran, Iran)
7–Manijeh Garooni MS,
Microbiologist , Laboratory of Imam Hossein Hospital, Shaheed Madani
Street , Shaheed Beheshti University of Medical Sciences and Health
Services ,(Tehran, Iran)
Key words:
anthrax, child
Abbreviated title:
intestinal anthrax
ABSTRACT:
Anthrax is the most fetal infectious disease that still,
because of incorrect and prompt diagnosis results to death.
Its intestinal form is the most severe and rarest one.
This article is about a 4- year old boy with abdominal pain and vomiting
and distention and bad general condition from a few days before admission
and was operated with a probability of peritonitis. Right hemicolectomy
because of ileocecal region invagination and perforation was done but
four hours later, the patient died with septic shock.
This article tries to demonstrate the importance of
epidemiological control of this disease that todays is on the world
concern, besides awareness of necessary implications for prompt diagnosis
and treatment can save the patient life.
INTRODUCTION:
Anthrax is caused by a gram negative
anaerobic bacillus which lives in soil. It affects animals such as cow,
sheep, horse, goat and pig. Human transmission occurs by direct (with
animal meat and blood ) and indirect ( with animal hair and wool) contact.
Anthrax affects skin , lung , and GI tract and all these three forms can
involve CNS . Skin form is the most common and GI form is the rarest (1).
There are a few reports of intestinal anthrax in literature: an eleven
year old girl with GI and CNS form from Poitzer (France)(2), a 2 year old
Iranian child with GI form (3), a 20 year old woman with GI form (1970)
(4). In addition to bioterrorism , world trade system and international
products transport from andemic places is still an important threat .
CASEREPORT: :
a 4 year old boy was admitted at
August 11 , 2002 in Imam Hosein Hospital (TEHRAN,IRAN) , he had a history
of a two days gradual abdominal pain and distention with constipation and
one day vomiting and fever . There was no family history of a disease but
a suspicious contact with a dead animal was detected. Axillary temperature
was 38.5 c , systolic pressure 110 mmHg , RR 45/min
and PR 125/min , he had an ill appearance , bowel sounds were hypoactive .
In rectal examiunation there was normal stool
without obvious blood , kernig and brudzinsky signs were negative , blood
specimen was sent to laboratory and Antibiotic therapy with Amikacin ,
Clindamycin and Ceftriaxone was started . Chest XRay was normal. Plain
abdominal X ray showed midposition of gut because of ascitis and edematous
luminal boarders . Abdominal sonography showed liver nodularity and
extensive ascitis , bowel loops expansion with fluid and gas but there was
no organomegally. A specimen was aspirated from the ascitis which had a
pussy appearance , gram strain preparation showed a lot of WBC and RBC
with gram positive bacillus . (table 1 )
Table 1 –
Lab. Results from the patient with GI Anthrax in IMAM HOSEIN Hospital
(Tehran – Iran )
|
Laboratory examination |
Results |
|
blood |
Hgb (gr/dl) |
16.6 |
|
WBC (mm3) |
41000 |
PMN %78 |
|
Biochemistry |
Urea (mg/dl) |
72 |
|
Na (meq/lit) |
120 |
|
K (meq/lit) |
5 |
|
Ca (meq/lit) |
9.3 |
|
Creatinine |
0.9 |
|
Ascitis |
WBC (mm3) |
4200 |
PMN %85 |
|
RBC (mm3) |
4700 |
|
U/A |
WBC (mm3) |
1-2 |
|
S/E |
WBC (mm3) |
25-30 |
|
RBC (mm3) |
20-25 |
|
Blood and ascitis fluid was sent for smear and culture .
After one hour of admission and in concern to progressive abdominal
distention and rebound tendernerness and laboratory results , acute
surgical abdomen and peritonitis secondary to bowel lumen perforation was
suspected and elective laparatomy was done , after midabdominal incision
2-2.5 litre fluid poured out and ileocecal intussusception was detected
and extensive necrosis and perforation was detected . a right
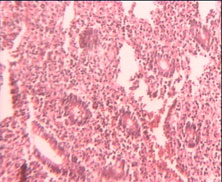
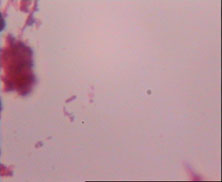
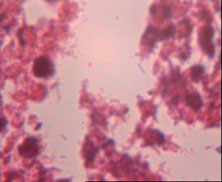
hemicolectomy and small bowel resection was done . In pathologic
examination, edema and necrosis and intestinal perforation and
colonization of gram positive organisms on perforation site was seen .
There was 40 acute suppurative adenopathy in paracecal and ileal region
(figure2,3 ).
After operation the patient admitted to ICU and
ampicillin ,amikacin and metronidazole was started . By the way pulse rate
reduction not responding to drug therapy and hypotension occurred and the
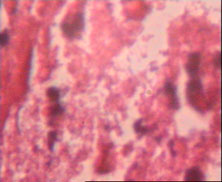
patient died with septic shock. On blood and acsitis smear preparation
there was a lot of gram positive bacillus with ellipsoidal central
endospores . Specimens cultured on blood agar and after 18 hours of
incubation colonies appeared with irregular boarders and 5 mm width ,
smear from colonies showed gram positive bacillus with smooth ellipsoid
central boarders(figure4), on secondary culture on sheep agar there was no
hemolysis , organism had no movement , it was lecithinase positive on egg
yolk agar , no acid formation from salicin, nitrate positive, endole
negative, gelatin hydrolysis after seven days was positive and it was
sensitive to penicillin (10IU). These LAB examinations were done in
REFERENCE laboratory (Tehran – Iran)
And diagnostic confirmation was done in RAZI institute of
research .(Tehran – Iran)
DISSCUSSION:
Anthrax has a known cycle in nature including 1 – spores multiplication in
soil 2- animal infection and 3 – human infection(1).
With PH increasing to more than 6 and supplementation
with (animal waste) and after intermittent rainfall , spores become
activated and multiply . important factor in epidemiology and disease
control is viable spores persistance for a few decades .
Yearly report of this disease is200-2000 cases but there
are cases that are not reported . Three forms of disease (skin more than
95% ) and GI and respiratory form exists . Because of animal control and
vaccination , the disease is very rare in USA . Meanwhile it is endemic in
Iran , Turkish , Pakistan and Sudan and after domestics infection , human
disease and GI anthrax (by infected meat consumption) is possible.There
are important factors for effective diagnosis and treatment , skin form is
easily distinguishable by the black central scar but GI form based on
bowel or pharyngeal involvement may have signs as bloody vomiting , melena
or bloody diarrhea, bloody pussy ascitis , erythematous cervical
lymphadenitis and edema and disphagia(5). In nontreated cases there is
sever toxicity , intestinal perforation , peritonitis or in our patient
intussusception caused by ileal adenopathy . He had no history of bloody
vomiting or stool but tense ascitis and abdominal distention was found.
Because of nonspecific signs and rareness this disease cannot be placed in
differential diagnosis (6). Direct ascitis and pleural fluid smear and
blood culture is helpful. Titer rising 3 to 6 months after beginning of
illness can be detected. GI Anthrax should be differentiated from duodenal
ulcer , thyphoid and tularemia(5). Penicillin is used for systemic and
skin form and in meningitis streptomycin and ciprofloxacine is added .
Treatment period is 14 days but because of diagnosis delay it was not
recommended for our patient . Mortality in GI form is more than 50% and
more than 100% in respiratory form(5). Awareness of anthrax signs and
symptoms , having clinical suspection and appropriate treatment by
penicillin or in cases of hypersensitivity , erythromycin , ciprofloxacin
or tetracycline increases treatment success. High risk people vaccination
is recommended and prophylaxis by penicillin till 7 days after contact
with bacillus is beneficial (5).
CONCLUSION:
Anthrax is endemic in Iran ,
therefore it should be suspected in cases of GI and respiratory tract
bleeding or sever peritonitis and septicemia in people in contact with
domestic animals and their products . because of high sensitivity of this
organism to penicillin , it can be used with 400000IU/kg in 4 to 6 divided
doses and in combination with other drugs .careful report of disease and
identification of endemic sources and domestic animals ans their
vaccination , use of detergents such as formaldeid (1) are done to
disinfect the soil .
REFERENCES:
1–Koneman EW, Allen DS, Janda WM,
Schreckenberger PC, Winn WC, Color Atlas and Textbook of Diagnostic
Microbiology, 5th edition, Philadelphia , Lippincott
2 - Berthier M, Fauchere JL,
Perrin J, Grignon B, Oriot D. fulminant meningitis due to bacillus
nthracis in 11 year old girl during Ramadan, The Lancet 1996; 347:828
3-Alizad A, Ayoub EM, Makki N.
Intestinal anthrax in a 2-year-old child, The Pediatric Infectious Disease
Journal 1995; 14(6): 394-5
4 - Nalin DR, Sultana B. Survival
of a patient with intestinal anthrax, Am J Med 1997; 62:130-2
5 - Edwards MS. Anthrax In: Feigin
RF, Cherry JO eds. Textbook of pediatric infectious disease, 3rd
edition. Philadelphia: Saunders, 1992
6 - Friedlander AM, Clinical
Aspects, Diagnosis and treatment of Anthrax, J Appl Microbiol 1999; 87(2):
303
|