|
پروفسور محمد حسین سلطان زاده
استاد
دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
دکتر
علی
رضا فهیم زاد
فوق
تخصص عفونی اطفال
دکتر
شهناز ارمین
فوق تخصص
عفونی اطفال
به اتفاق اعضای هیئت علمی بخش تحقیقات عفونی بیمارستان مفید
دکتر پیمان عشقی
فوق تخصص خون اطفال بیمارستان مفید
شرح حال توسط
دکتر عباس
بسکابادی
رزیدنت مفید |
معرفی بیمار
Case presentation
اهل و
ساکن : پارس آباد مغان استان اردبیل
نژاد:
ترک
شرح حال
دهنده : پدر و مادر بیمار( پدر آشنا به زبان فارسی و مادر ترک زبان)
PI:
بیمار
پسر8 ماهه با شکایت تب و زردی مراجعه کرده است.
مشکل
بیمار از حدود 40 روز قبل از مراجعه به این مرکز با بی قراری و تب شروع شده است. تب
بیمار در این مدت پایدار بوده، با استامینوفن کنترل میشده است ولی مجددا عود میکرده
است. بیمار تحت درمان های سرپایی متنوع قرار گرفته که بهبودی حاصل نشده است. بتدریج
از حدود 1 ماه قبل دچار دیستانسیون شکمی و ادم اندام ها و ایکتر می شود که پیشرونده
بوده است. بدنبال آن با شکایت تب طول کشیده و دیستانسیون پیشرونده شکمی در
بیمارستان پارس آباد بستری می شود. که یک شب در آن جا بستری بوده و با رضایت شخصی،
پدر فرزند را به بیمارستان اردبیل منتقل می کند. طبق موارد ذکر شده در بیمارستان
اردبیل بررسی هایی در آن جا انجام می شود که بطور خلاصه عبارتند از:
بیمار
دچار هپاتواسپلنومگالی به همراه آسیت و افیوژن پلورال است.
نتایج
آزمایشات اولیه :
Bil T:
5.2, Bil D: 3.7, SGOT: 1016, SGPT: 3680
پاراسنتز مایع پلور انجام نشده است.
جهت
بیمار در آن مرکز درخواست انجام
BMA
می شود که پدر بیمار رضایت به انجام آن نمی دهد. بدنبال آن بیمار با شک به لشمانیوز
احشایی تحت درمان با گلوکانتیم قرار می گیرد، که پس از 4 روز بدنبال عدم بهبودی در
وضعیت بیمار، با رضایت شخصی از آن مرکز خارج و به بیمارستان مفید مراجعه می کند.
PMH:
بیمار
فرزند دوم از مادر
G2P2Ab0
می باشد. حاصل زایمان ترم و سزارین ( بعلت آسپیراسیون مکونیوم)
بمدت 1
هفته بدنبال آن در بیمارستان بستری بوده است.
سابقه
بستری و بیماری همراه دیگری را نمی دهد. دیگری را نمی دهد.
بیمار
از لحاظ رشد و تکاملی نرمال است.
F.H:
پدر و
مادر بیمار منسوب نمی باشند.
خواهر 3
ساله بیمار سالم و مشکلی ندارد.
سابقه
بیماری خاصی در خانواده نمی دهد.
D.H:
گلوکانتیم به مدت 4 روز
آنتی
بیوتیک ( پنی سیلین،اسامی بقیه را بخاطر نمی آورد)
Ph/Ex:
بیمار
در هنگام مراجعه هوشیار،
ill
بود ولی توکسیک نبود.
BP:
90/70(mm.Hg) PR:108/min
با
استامینوفن
RR: 25/min AT: 37.1c
سروگردن:
فونتانل
قدامی 0.5*1
cm
باز بود. فونتانل خلفی بسته بود.
صورت
دیسمورفیک نداشت.اسکلرا ایکتریک و ملتحمه
pale
بود.
معاینه
گوش ها و دهان نکته خاصی نداشت.لنف نود گردنی نداشت.
قفسه
صدری:
دفورمیتی قفسه صدری نداشت.اکسپانسیون قفسه سینه نرمال و قرینه بود.
رتراکسیون ساب کوستال و اینترکوستال نداشت.سمع ریه ها دوطرفه
clear
بود.
سمع قلب
S1و
S2
سمع شد سوفل یا صدای اضافی شمع نشد.
شکم:
در نگاه
دیستانسیون واضح دارد. دفورمیتی یا اسکار جراحی ندارد.صدای روده ای بصورت نرمال سمع
می شود.در لمس کبد حدود 6
cm
زیر لبه دنده ای بدست می خورد، با قوام نرمال. (
span=10
cm)
لبه کبد
نیز حدود 4
cm
زیر لبه دنده ها بدست می خورد.در دق ماتیته در پهلوها و تمپان در وسط شکم در حالت
supine
دارد.
Shifting dullness
در معاینه دارد.
ژنیتالیا:
نرمال
پسرانه و ختنه شده. بیضه ها داخل اسکروتوم لمس می شوند.
اندام
ها:
نبض ها
بصورت پر و قرینه لمس می شود.دفورمیتی در اندام ها ندارد.
مشکل
حسی ی حرکتی ندارد.
در
دیستال اندام تحتانی ادم
pitting
در حد ساق پا وجود دارد.
LAB
10/26
CBC
WBC:
3600 poly: 15% lymph:83%
HGB:
13.1 MCV:79 MCH: 25.7
MCHC:32
Plt:
43000
BS:202, BUN:5, Cr:0.5, Na:133, K:4.1, Ca:9.6,
SGOT:202, SGPT: 127, Bil T: 9.1, Bil D: 2.1
Uric
acid: 2.8, CRP: 3+, PT:25, PTT: 55,
Total
Pr: 3.8, Alb:2.1, Widal: negative
Blood
culture: pseudomonas
10/27
Hb A:
95.7%
Hb F:
1.9%
Hb A2:
2.4%
Direct
combs: negative, Cold agglutination: negative
Pyruvat:
3.1 (0.3-0.7), Lactate: 51 (4.5- 20)
Amunia:
101 (27.2-102)
Urine
reducing substance: positive
Urine
amino acid: normal, Blood amino acid: normal
11/2
Cholesterol: 121, TG: 218, Ferritin: 750
Fibrinogen< 94
11/3
Blood
culture: negative
11/6
Galactomannan: 0.3(negative)
Bone
Marrow Aspiration
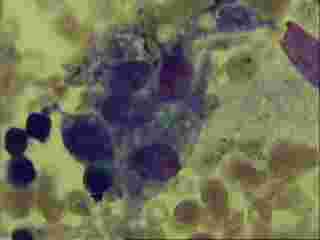

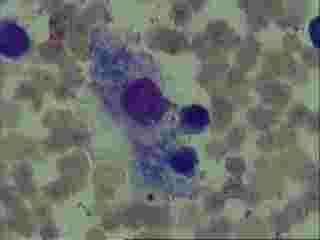
BMA
Mild to
moderate hypo cellular. Hemophagocytosis were seen.

CXR
Cardio thoracic
ratio is in normal range .
bilateral
hyperaeration with reticular opacities is evident .
Costophrenic
angles are clear
Soft tissue and
bone densities of the thorax are unremarkable.
10\26
Abdominopelvic
ultrasound :
Liver is
enlarged (mild hepatomegaly)and homogenous echopattern.( 109 mm)
No space
occupying lesion is seen.periportal echogenisity is increased.
Gall bladder has
normal wall thickness and echo free content.
Intra and extra
hepatic bile ducts, CBD and portal vein have normal caliber.
Bilateral kidneys
have normal size and cortico medullary echo pattern and differentiation.
( RK 65mm,
LK = 66 mm)
Bilateral renal
cortical thickness are normal.
There is no
evidence of hydronephrosis or renal calculi.
Pancreas has
normal echo texture. Para aortic regions are unremarkable.
Spleen is
enlarged and multiple target lesion with isoecho center and hypoecho rim with
19*16 mm in gerater diameter throught the spleen are seen. ( 83 mm)
DDX:infection such as cadidiasis or lymphoma
Urinary bladder
has normal wall thickness with echo free content.
No evidence of
stone or vegetative lesion is seen.
Pelvic organs are
unremarkable
No abnormality in
pelvic cavity is seen.
moderate ascitis
in abdominopelvic cavity is seen.
no plural
effusion is seen.
Bone Survey


Bone survey :
Bone density is
decreased .
There is no
evidence of lytic or sclerotic lesion.
Fracture or
dislocation is not seen
Soft tissue
density around mentioned bones is unremarkable.
10\29
Abdominopelvic
ultrasound :
Severe ascitis
is seen in abdominopelvic cavity.
Liver has
enlarged(CC span:112mm)but has homogenous echopattern.
No space
occupying lesion is seen.
Gall bladder has
increased wall thickness that might be due to ascitis.
It fills with
anechoic fluid.
Intra and extra
hepatic bile ducts, CBD and portal vein have normal caliber.
Bilateral kidneys
have normal size and cortico medullary echo pattern and differentiation.
( RK=76x32 ,LK
= 75x26mm)
Bilateral renal
cortical thickness are normal.
There is no
evidence of hydronephrosis or renal calculi.
Due to increased
abdominal bowel gas evaluation of oancreas and para-aortic region can nit be
done.
Spleen has
enlarged(84mm) and it has homogenouse echogenicity in general but multiple
target lesions are evident throughout splenic tissue.
the greatest
lesion is measured about 18*16 mm.
It may be due to
lymphomatouse mass lesion or oppurtunistic infections(especially fungal
infection).
Urinary bladder
has normal wall thickness with echo free content.
No evidence of
stone or vegetative lesion is seen.
Pelvic organs are
unremarkable
No abnormality in
pelvic cavity is seen.
Dr.Mahdavi
Brain spiral CT
scan with contrast media :
Brain parenchyma
has normal density.
Ventricular
system is normal.
No mass effect or
midline shift is seen in supra and infra tentorial region.
Posterior fossa,
CP angles , pons and midbrain are unremarkable.
No evidence of
hemorrhage or calcification is seen.
There is no
pathologic enhancement after administration of IV contrast in supra and infra
tentorial region
Spiral CT scan of
the thorax with IV contrast :
There is no
evidence of parenchymal lesion.
There is no
evidence of anterior, middle and posterior mediastinal mass. major vessels are
normal.
Hilar regions are
normal. Trachea and major bronchi have normal caliber.
No pathologic
enhancement after IV contrast is seen.
There is no
evidence of pathology in bony thorax and soft tissue thoracic wall.
bilateral Pleural
effusion is seen.
Abdominopelvic
spiral CT scan with IV and oral contrast media :
bilateral pleural
effusion is seen .
liver is enlarged
and has decreased density may be due to fatty changes.
there are several
hypodense nodules with rim enhancement in spleen.
abscess formation
should be considered.
Intra and extra
hepatic bile ducts and CBD are normal.
Pancreas is
noticed with normal position and density.
There is no
evidence of abnormality in size and density of both kidneys.
After IV
contrasts both kidneys excreted normally.
No evidence of
hydronephrosis or stone is seen.
There are no
pathologic findings in bilateral adrenal glands.
Omental and
mesentric fat planes are seen normally.
Pelvic organs are
seen without pathologic findings.
Urinary bladder
has normal wall thickness with regular borders.
Perineal and
perirectal and ischiorectal fat planes are normal.
No evidence of
space occupying lession in pelvis is seen.
ascitis is seen.
There is no
pathologic enhancement after administration of IV contrast in abdominopelvic
region.
تشخیص شما چیست ؟



