|
پروفسور محمد
حسین سلطان زاده
استاد دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
معرفی : دکترفریده
شیوا
به اتفاق اعضای هیئت علمی گروه کودکان
بیمارستان طالقانی
|
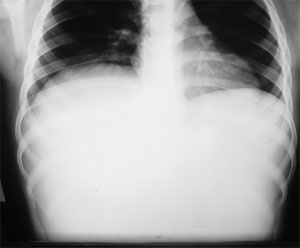
22/02/1386.
Liver & spleen scan by
99m-Tc phytate:
Angiography multiple
smallzones
with high blood flow
detected.
Static phase
demonstrated
a hugely enlarged liver
which was
occupied by a loculated
mass with
no uptake of
radiotracer.
Impression:
Hepatomegaly with a huge space-occupying lesion
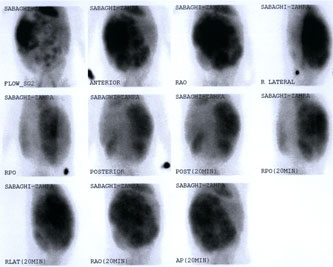
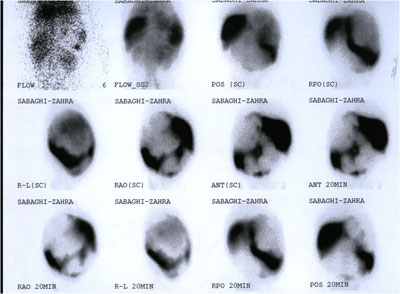
Tc 99m-RBC scan:
Liver is occupied by a very
huge mass which
revealed gradual accumulation
of RBC-labeled radiotracer.
Impression: Scan is in favor
of a
very huge and loculated
hemangioma
with
probable AV malformation
inside the lesion.

Liver Hemangiomas
Hemangiomas are benign tumors
of the endothelial cells which normally line the blood vessels.
Approximately 60% hemangiomas
-- head and neck
about 25% -- trunk, 15% arms
or legs.
Most (about 80%) hemangiomas
grow as a single tumor, about 20% multiple areas.
nHemangioma
is most common benign tumor of the liver (0.4-7.3% incidence at
autopsy)
nSizes
range from 2 mm to more than 20 cm.
ntypically
measure less than 5 cm; larger than 4-5 cm are called giant hemangiomas
(Cappellani, 2000; Yang, 2001).
Natural history of liver
hemangioma
not completely understood.
Probably congenital in origin.
Several pharmacologic agents
have been postulated to promote tumor growth.
Steroid therapy, estrogen
therapy, and pregnancy increase the size
of already existing hemangioma
nUsually
solitary lesions.
nmay
be multiple in as many as 50% of patients (Mergo, 1998).
n
nNo
lobar predilection.
nHemangiomas
are uncommon in cirrhotic livers; the fibrotic process in cirrhotic liver
may
prohibit their development . (Dodd, 1999).
Clinical Presentation
nSex:
female-to-male ratio of 5:1 to 6:1.
nAge
: can occur in
individuals of any age.
frequently occur
in middle-aged women.
: Hepatic hemangiomas are
rare in infancy. (report of 2 infants, Kullendorff 2002,)
: Have been detected
prenatally in a growing fetus. (Gembruch, 2002. Pott Bartsch, 2003)
Physical examination:
enlarged liver.
an arterial bruit over the
right upper quadrant.
Lab Studies :
nResults
usually normal.
nAnemia
and reduced hematocrit levels in patients with ruptured hemangiomas.
nThrombocytopenia
-- from sequestration and destruction of platelets in large lesions.
nHypofibrinogenemia
has been attributed to intratumoral fibrinolysis.
nIn
patients with giant hemangiomas associated with Kasabach-Merritt
syndrome, bleeding and clotting parameters may be abnormal.
nNormal
alpha-fetoprotein and carcinogenic embryonic antigen (CEA) levels.
Complications :
nDepend
on the size / location of tumor.
nPressure
on the stomach and duodenum may cause vague abdominal pain, early
satiety, nausea, and vomiting. (Tran-Minh,
1991).
nPedunculated
hemangiomas may twist and cause acute abdominal
pain.
(Tran-Minh, 1991)
nCompression
of the inferior vena cava -- Budd-Chiari
syndrome. (Hanazaki, 2001)
n
Portal hypertension.
(Takahashi, 1997)
Acute thrombosis --- acute
inflammatory changes --- consumption coagulopathy, fever,
abdominal pain, abnormal liver function.
In one review, 32 case
reports of spontaneous rupture of hepatic hemangioma in patients
greater than 14 yo without trauma.
Spontaneous or
post-traumatic rupture is a catastrophic complication that occurs in about
1-4% of hemangiomas; with mortality rate, as high as 60%. (Cappellani,
2000)
Clinical Syndromes :
Klippel-Trenaunay-Weber
syndrome:
Hepatic hemangiomas plus
congenital hemiatrophy and nevus flammeus, with / without hemimeganencephaly.
Kasabach-Merritt syndrome:
Giant hepatic hemangiomas,
thrombocytopenia & intravascular coagulation.
Osler-Rendu-Weber disease:
Numerous small hemangiomas
of face, nares, lips, tongue, oral mucosa, GIT, and liver.
Von Hippel-Lindau disease:
Cerebellar & retinal
angiomas, with lesions in the liver and pancreas.
Multiple hepatic
hemangiomas reported in SLE.
Differential Diagnoses :
Other hypervascular benign
and malignant space-occupying liver lesions.
Benign lesions
cysts, adenomas, focal
nodular hyperplasia, and regenerating nodules.
Malignant lesions
hepatocellular carcinoma
and metastasis hemangioendothelioma.
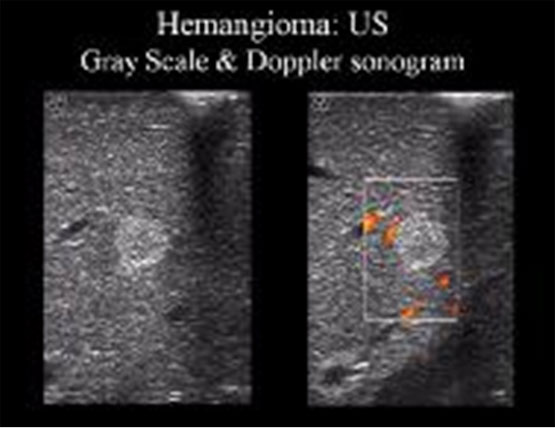
Ultrasonography is a
cost-effective imaging modality for diagnosis of a hemangioma.
CT and/or MRI may be
required to specifically diagnose hemangioma
Most commonly initial
diagnostic tool.
Usually homogeneous
Well-defined hyperechoic
masses (though few can appear relatively hypoechoic
when imaged within a fatty liver)
Giant lesions can appear
heterogeneous secondary to internal complex composition
Gray-scale and Doppler
sonograms show a well-defined, uniformly hyperechoic liver mass
with peripheral feeder vessels. These features are characteristic of a
hemangioma
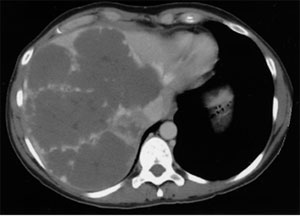
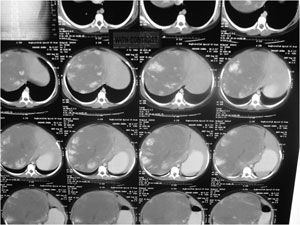
CT with sequential scans
Focal, well-circumscribed, low
attenuation lesions
on pre-contrast images
Nodular, peripheral
centripetal enhancement
on dynamic
contrast enhanced imaging

magnetic resonance imaging (MRI),
hepatic arteriography,
and
digital subtraction
angiography (DSA).
MRI :
nSensitivity
and specificity >90%
nDifferentiates
hemangiomas from other liver lesions
nTypically
hemangiomas are homogeneously hypointense relative to the liver on
T1-weighted and markedly hyperintense (lightbulb sign) on T2-weighted images
relative to the liver
nOn
dynamic, contrast-enhanced MR imaging, Peripheral, nodular centripetal
enhancement pattern progressing to homogeneity (lesions 1.5-5cm)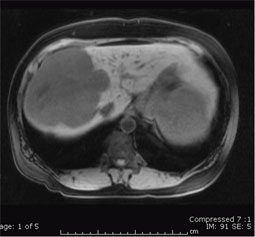
nPeripheral
nodular centripetal enhancement with persistent central hypointense region
(lesions> 5cm)
Giant cavernous
hemangioma
of the liver:
Axial T1-weighted pre-contrast
image
shows a hypointense mass within the right hepatic lobe.
Sequential enhanced delayed
images show
peripheral nodular centripetal enhancement with persistent central hypointensity
Tc-99m pertechnetate-labeled
RBC pool studies
used for many years.
For lesions that are greater
than 2 cm in diameter,
Sensitivity reported at 82%.
The specificity
is up to 100%
single-photon emission
computerized tomography
(SPECT) with colloid
99m-labeled RBCs.
Single-photon emission computerized tomography (SPECT)
–SPECT
with colloid 99m-labeled RBCs appears to be as sensitive and specific as MRI.
–At
present, SPECT scan is most likely the investigation of choice to confirm
the diagnosis of hepatic hemangioma.
–Hemangiomas
as small as 0.5 cm may be detected with SPECT.
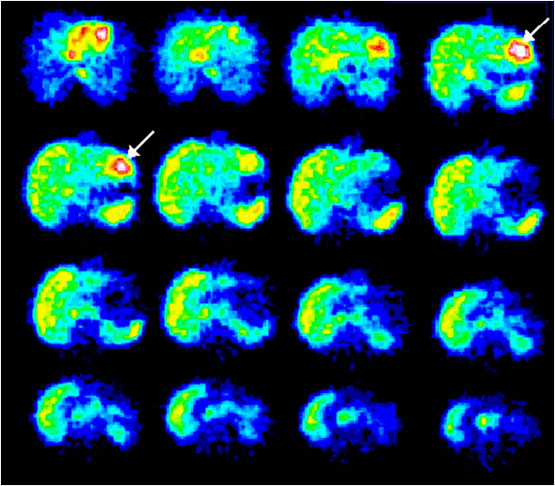
SPECT examination: Axial scans
of blood-pool scintigraphy with 99mTc-labeled erythrocytes: A well-circumscribed
area (arrow) of increased activity is present in the left lobe of the liver,
which indicates pathology with a high blood content.
Histologic Findings
Cavernous hemangioma are atypical or irregular in arrangement and size.
Microscopically:
Mesenchymal in origin.
composed of cavernous
vascular channels lined by single layers of flattened endothelium
and separated by fibrous septa.
These vascular spaces may
contain thrombin, calcifications, or prominent scarring with
hyalinization (sclerosed hemangioma).
Malignant transformation has
not been reported.
Enucleation/Resection
Transcatheter arterial
embolization, (polyvinyl alcohol particles)
Surgical ligation of feeding
vessels.
Radiofrequency ablation:
Percutaneous & laporoscopic
radiofrequency ablation
to improve abdominal pain.
Hepatic irradiation:
With a dose of 30 Gy in 15
fractions for3 weeks
reported to produce complete
regression of hemangiomas.