|
پروفسور محمد
حسین سلطان زاده
استاد دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
دکتر مینو فلاحی
فوق تخصص نوزادان
استاد یار دانشگاه علوم
پزشکی شهید بهشتی
به اتفاق اعضای هیئت علمی گروه کودکان
بیمارستان
شهدای تجریش |
تشخیص
}
Choanal atresia
}
Most
common congenital anomaly of the nose
}
1/7000
live birth
}
Unilateral
or bilateral
}
Bony(90%)
or membranous(10%) septum between nose and pharynx
}
Most cases
:combination of bony and membranous
}
20-50%
with other congenital anomaly(more frequently in bilateral form)
}
CHARGE
association(Coloboma ,Heart disease ,Atresia choanal ,Retarded growth and
development or CNS anomaly ,Genital anomaly or hypogonadism ,Ear anomaly or
deafness
}
Clinical manifestation of choanal atresia:
}
Variable
ability to breathe in neonates through month
}
Unilateral
form: asymptomatic for a long period by a nasal discharge or persistent
obstruction
}
Bilateral
form: symptomatic in neonatal period
}
Diagnosis of Choanal atresia
}
Inability
to pass a firm catheter through each nostril 3-4 cm into the nasopharyinx
}
Fiberoptic
rhinoscopy
}
High
resolution CTS
}
Differential diagnosis:
}
Congenital
defect in nasal septum
}
Stenosis
of pyriform apertus
}
Congenital
midline nasal mass:dermoid.gliomas,encephalocele,hemangiomas,congenital
nasolacrimal duct obstruction.nasal polyp,tumor(rhabdomyosarcoma)
}
Treatment of choanal atresia
}
Prompt
placement of oral airway
}
Feeding by
gavage
}
Intubation
or tracheostomy
}
Trans
nasal repair(stent for weeks) in 4-6wk or body weight of 4 kg
}
Unilateral
atresia:infancy(4-5yr)
}
Case presentation
}
A 1800 g
preterm (36 weeks) male was born to a G3 mother by NVD. The baby cried
immediately after birth and there was no perinatal asphyxia. Soon after birth
the baby developed respiratory distress with mild cyanosis. Attempts to pass a
nasogastric tube through the nose were un-successful. Esophageal atresia was
ruled out by passing an oro-gastric tube. A provisional diagnosis of bilateral
choanal atresia was made.
}
Routine
laboratory investigations were normal. The chest X-ray and X-ray
naso-pharyngeal region lateral view did not show any abnormality. Ultrasound
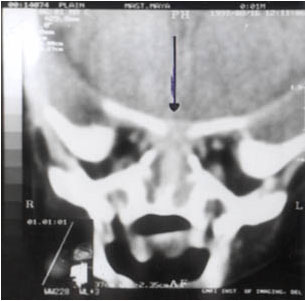
cranium was normal. A CT scan of the paranasal sinus region and skull showed a
bony defect in the floor of anterior cranial fossa in the region of the
cribriform plate with brain parenchyma extend-ing into the nasoethmoidal region
(Fig.). These findings suggested the diagnosis of trans-ethmoidal
encephalocele as the cause of nasal obstruction.
}
bony
defect in cribriform plate and protruding brain tissue (arrow).
}
Risk factors
}
Race
}
Encephaloceles have a multifactorial etiology, and genetic and geographic
factors have been implicated. Frontal encephaloceles are far more common in the
Far East, particularly in the Chinese population, and are associated with a more
favorable prognosis.
}
Sex
}
Encephaloceles occur more commonly in females than in males.
}
Age
}
Currently,
most encephaloceles are diagnosed prenatally and present at birth.,
Some, particularly sphenoidal encephaloceles, may become apparent later in
childhood.
}
encephaloceles
}
Occipital
in ¾ of cases
}
Frontal
(protrusion into the nasal cavity)
}
Rarely
:temporal or parietal



}
Anterior
encephalocele :infrequent (15–20% of the cranial encephaloceles)
}
1in 35,000
live births
}
the
incidence is much higher in Southeast Asian countries, including some parts of
India(it is as high as 1:5,000 live births in Thailand.)
}
Transethmoidal encephaloceles (TEE), a subtype of basal anterior encephalo-cele,
is the protrusion of a part of brain tissue through a bony defect in the
cribriform plate into the anterosuperior nasal cavity.
}
Types of Basal anterior encephaloceles
}
depending
on the site of the bony defect :
}
Sphenoethmoidal
}
, trans-ethmoidal,
}
transphenoidal
}
spheno-orbital.
}
Naso-frontal,
naso-ethmoidal and naso-orbital or combination of these.
}
Frontoethmoidal encephaloceles are the commonest type,
}
Frontoethmoidal encephaloceles :commonest type, followed by the nasopharyngeal
and orbital type.
}
Among the
frontoethmoidal encephaloceles, nasoethmoid is the commonest type, (swelling
over the bridge of the nose with significant hypertelorism and orbital
deformities)
}
The
nasopharyngeal type remains occult and presents with nasal obstruction or CSF
rhinorrhea. Rarely, the patient may present with meningitis.
}
There was
associated hydrocephalus and agenesis of the corpus callosum
}
Clinical manifestation
}
signs and
symptoms of nasal obstruction mimicking choanal atresia
}
,
hyperteleorism,
}
CSF
leakage
}
recurrent
meningitis
}
orbital
deformities
}
hydrocephalus
}
The
aware-ness of this lesion in differential diagnosis of choanal atresia is of
practical importance because failure to recognize this lesion can lead to
surgical misadventure. The advent of CT scanning and MRI has made the diagnosis
simple. These scans help to delineate the extent and characteristics of the
anomaly.
}
The aim of
surgery is to excise the encephalocele, repair the dural defect and correct the
facial and orbital deformity. The ideal age for surgery is around 6-9 months.
Early surgery leads to better cosmetic results and prevents CSF leak.


