|
پروفسور محمد حسین سلطان زاده
استاد
دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
خانم
دکترزهرا
پورنصیر
به اتفاق اعضای
هیئت علمی گروه کودکان
بیمارستان لقمان
دکتررضا
امیر عسگری
رزیدنت بیمارستان مفید
دکتر قاسم سعیدی
انترن
بیمارستان مفید |
خانم
دکترزهرا
پورنصیر
Differential diagnosis of multiple pulmonary nodules
Infection
Abscesses:Bacteremic
patients and recurrent aspiration may develop multiple lung abscesses, which
are more common in dependent areas of the lungs. Typically the lesions are
between 0.5 and 3 cm in diameter, round, and well-defined.
Septic emboli : predilection
for peripheral areas of the lower lobes
Fungi : histoplasmosis,
coccidioidomycosis, cryptococcosis, or invasive aspergillosis in
immunocompromised hosts.
Histoplasmosis
Symptomatic pulmonary
histoplasmosis :
subacute pulmonary
infection weeks to months following exposure. Symptoms are usually mild, and the
events causing the exposure are difficult to identify. Radiographs typically
show focal infiltrates and mediastinal or hilar lymphadenopathy .
Acute diffuse pulmonary
histoplasmosis :
the majority of patients
develop acute symptomatic infection within a week or two .Diffuse
reticulonodular or miliary pulmonary infiltrates are noted and the disease can
progress to respiratory failure or progressive extrapulmonary dissemination
Chronic pulmonary
histoplasmosis:
Patients susually have
underlying lung disease. Affected patients develop a productive cough, dyspnea,
chest pain, fatigue, fevers, and sweats and have fibrotic apical infiltrates
with cavitation on chest radiographs or CT scans .
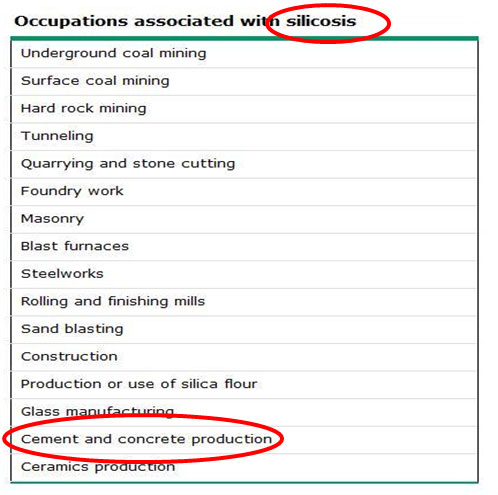
Silicosis
Silicosis refers to a
spectrum of pulmonary diseases caused by inhalation of free crystalline silica
(silicon dioxide).
Silicosis can occur in many
industries and work settings including mining, quarrying, sandblasting, masonry,
foundry work, and ceramics
Several clinical
presentations of disease have been described
Chronic silicosis: usually
appearing 10 to 30 years after first exposure
Accelerated
silicosis:Accelerated silicosis develops within 10 years of initial exposure.
Accelerated silicosis is associated with high-level exposure to silica.
Acute silicosis : Acute
silicosis is characterized by rapid onset of symptoms including cough, weight
loss, fatigue, and sometimes pleuritic pain.
Inflammatory conditions
Wegener's granulomatosis,
rheumatoid arthritis, Pulmonary lymphomatoid granulomatosis, amyloidosis, and
sarcoidosis.
Sarcoidosis presents in
patients between 10 and 40 years of age in 70 to 90 percent of cases.
Younger children often
present with skin rash, arthritis, and uveitis without apparent lung involvemen.
The "classic" chest roentgenogram reveals bilateral hilar adenopathy
Pulmonary
AVMs
Malignancy :Non-Hodgkin
lymphoma , choriocarcinoma, renal cell carcinoma, melanoma, thyroid carcinoma
and Kaposi's sarcoma,
pulmonary alveolar
proteinosis
Desquamative interstitial
pneumonia (DIP)
Lymphocytic interstitial
pneumonia (LIP)
Miliary tuberculosis (TB)
PULMONARY
ALVEOLAR MICROLITHIASIS
A rare idiopathic lung
disease characterized by the presence of innumerable tiny calculi (microliths)
composed primarily of calcium phosphate within alveolar air spaces.
It was not well characterized
until the 1950s. Since then, interest in the disease (and the number of reports)
has increased; in 1957 one report described 26 cases, and by 2005, 576 cases had
been reported in the literature.
Pulmonary alveolar
microlithiasis most frequently appears in Turkey, followed by Italy.
The disease can occur in
individuals of any age and has been reported in stillborn twins and an
80-year-old woman.
However, it occurs most
often in adults between the ages of 30 and 50.
The familiar incidence of PAM
is reported,and in more than one half of the reported case a familiar incidence
has been demonstraed
PATHOGENESIS
The etiology and pathogenesis
of PAM are unknown.
Hypothetical mechanisms that
have been postulated include an inborn error of metabolism, a response to a
pulmonary insult or inhaled agent, and an acquired abnormality of calcium or
phosphorous metabolism or a environmental factor
PAM has been reported in
association with inhalation of various materials (e.g., mica, calcium-containing
snuff, or sand)
Mutations
in the SLC34A2 Gene Are Associated with Pulmonary Alveolar Microlithiasis
Homeostasis of inorganic
phosphate in the human body is maintained by regulated absorption, metabolism,
and excretion. Sodium-dependent phosphate transporters (NaPi) (mutation in the
SLC34A2 gene) mediate the transport of inorganic phosphate (P(i)) in cells in
response to dietary phosphate consumption, hormones, and growth factors.
Signaling pathways activated
by mitogens, glucocorticoids, and metabolic factors have been implicated in
regulating P(i) transport via NaPi2b.
Inactivation of NaPi2b
function by mutations has been linked to human pathologies, such as pulmonary
alveolar microlithiasis.
CLINICAL
PRESENTATION
Children with PAM are usually
asymptomatic
chronic cough : is
usually nonproductive, but sputum may be present and can contain microliths
Hemoptysis
dyspnea on exertion
Chest pain
clubbing
A number of cases have
been identified by radiologic evaluation of asymptomatic relatives of an
index case.
The physical examination
is usually unremarkable in children and even in adults unless the disease is
very advanced. In the late stages, tachypnea may be present and auscultation
of the chest may reveal diminished breath sounds
DIFF DIAG
PAM must be differentiated
from diffuse pulmonary calcinosis, which can be seen in :
hyperthyroidism,
chronic renal disease,
and vitamin D
intoxication.
PAM must also be
differentiated from:
Miliary tuberculosis
Disseminated
histoplasmosis
Hemosidrosis
PAM has been found in
association with cases of milk alkali syndrome , mitral stenosis , in a renal
transplant recipient , Primary ciliary dyskinesia (PCD)
NATURAL
HISTORY
Such reports suggest that the
disease begins with involvement of the lung bases and progresses slowly, toward
involvement of a progressively larger fraction of the lungs, leading ultimately
to death from respiratory failure, usually in early adult life.
In contrast, the disease can
be stable for long periods (up to 30 years in some patients), even when
extensive radiographic changes are present initially.
Pneumothorax can occur,
presumably from bullae and subpleural cysts, and can be recurrent in some
patients.
DIAGNOSIS
The diagnosis is usually made
by the charactreistric sandstorm on CXR
The HRCT can be helpful
Bronchoscopy with
bronchoalveolar lavage may reveal the presence of microliths in the lavage fluid
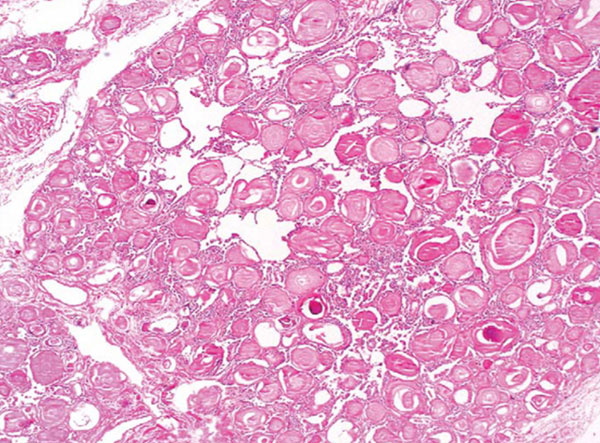
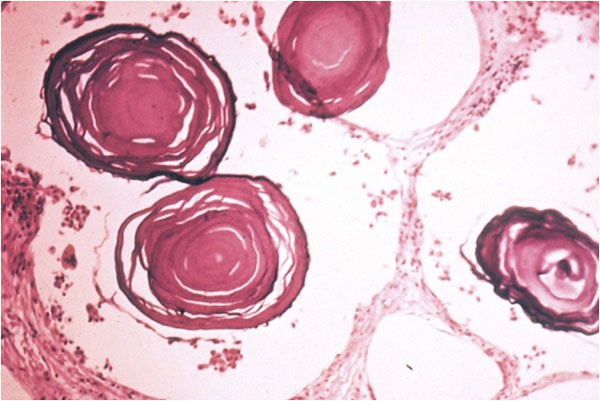
Transbronchial biopsy reveals
characteristic microliths that measure in diameter from 0.1-0.3 mm and are
located almost invariably within alveolar air spaces.
Occasionally, microliths are
present in the bronchial wall or interstitium and, rarely, in extrapulmonary
sites (e.g., in the seminal vesicles, sympathetic ganglia, or gonads,kidney).
THERAPY
No effective medical
therapy, and affected individuals may progress to end-stage lung disease
requiring lung transplantation.
Therapeutic methods
including systemic corticosteroids and bronchoalveolar lavage have been
shown to be ineffective
Diphosphonates(etidronate
disodium)
monoclonal antibodies specific for the human sodium-dependent phosphate
co-transporter NaPi2b

دکتررضا
امیر عسگری
دکتر قاسم سعیدی
A 7-year-old man with fever, dry cough& abnormal CXR
Diffuse
micronodular infiltrations
Pneumoconiosis
Silicosis
Asbestosis
Coal worker
Pneumoconiosis
Alveolar form of
sarcoidosis
TB (milliary)
Hypersensitivity
pneumonitis (extrinsic allergic alveolitis)
Fungal disease
Connective tissue disease
SLE,RA,wegner,MCTD,SS,Polymyositis,dermatomyositis,PAN,churg struss
Drug induced
Diffuse interstitial
fibrosis
Radiotherapy
Pulmonary alveolar
microlithiasis
…
Pneumoconiosis
Silicosis
Asbestosis
Coal worker
Pneumoconiosis
Alveolar form of sarcoidosis
Miliary TB
Hypersensitivity pneumonitis
(extrinsic allergic alveolitis)
Fungal disease
Connective tissue disease
SLE,RA,wegner,MCTD,SS,Polymyositis,dermatomyositis,PAN,churg struss
Drug induced
Diffuse interstitial fibrosis
Radiotherapy
Pulmonary alveolar
microlithiasis
…
Pericardial
calcification
Constrictive pericarditis
Prior episode of Pericarditis
or trauma
Infectious etiologies for
pericarditis
viral agents (eg,
coxsackievirus, influenza A, influenza B, varicella),
Tuberculosis
Histoplasmosis
Radiotherapy
CRF (uremic pericarditis)
systemic lupus erythematosus,
rheumatic heart disease
hemopericardium (post trauma
or cardiac surgery).
myocardial infarction
Occasionally, pericardial
tumors, such as intrapericardial teratomas
…
Pericardial
calcification
Constrictive pericarditis
Prior episode of Pericarditis
or trauma
Infectious etiologies for
pericarditis
viral agents (eg,
coxsackievirus, influenza A, influenza B, varicella),
Tuberculosis
Histoplasmosis
Radiotherapy
CRF (uremic pericarditis)
systemic lupus erythematosus,
rheumatic heart disease
hemopericardium (post trauma
or cardiac surgery).
myocardial infarction
Occasionally, pericardial
tumors, such as intrapericardial teratomas
…

Diffuse
micronodular infiltrations + Pericardial calcification
TB
Fungal disease
Viral agents
CTD
Systemic lupus erythematosus
Rheumatic heart disease
TB
Fungal disease
Hypersensitivity pneumonitis


