|
پروفسور محمد حسین سلطان زاده
استاد
دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
آقای دکتراحمد خالق نژاد
فوق تخصص جراحی اطفال و
استاد دانشگاه
بیمارستان مفید
مرکز تحقیقات جراحی اطفال بیمارستان مفید
دکتر سید محمد هادی امامی فر
رزیدنت بیمارستان مفید
دکتر محسن سنجری
رزیدنت بیمارستان امام حسین |
تشخیص
Late
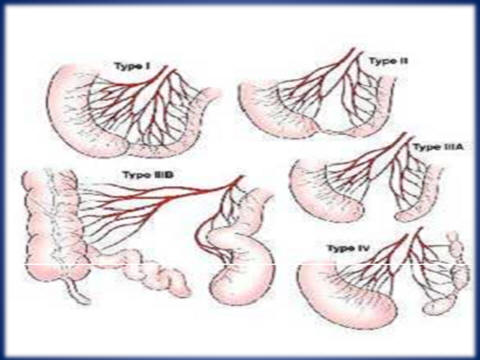
Jejunoileal atresia
دکتراحمد خالق نژاد
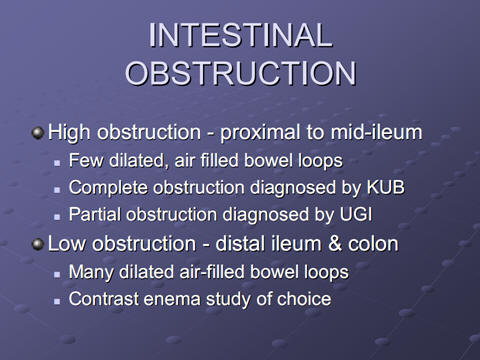
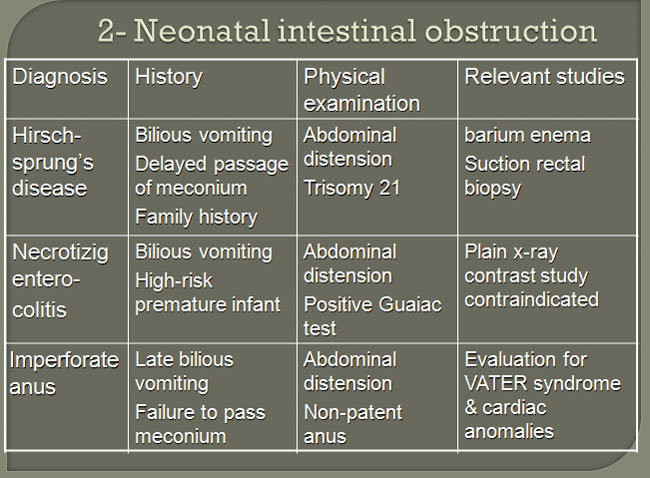
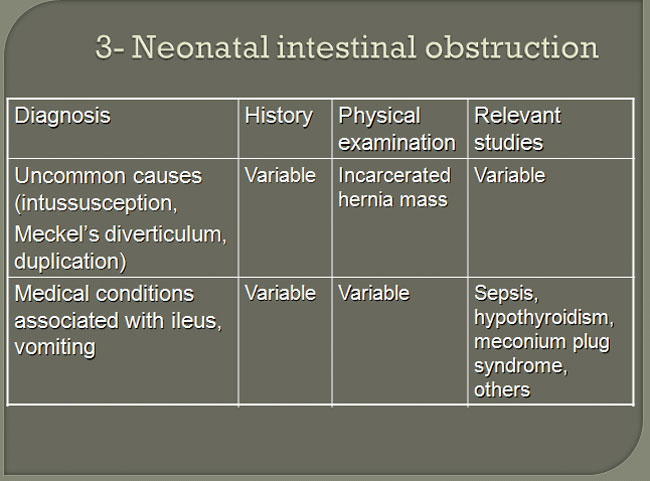
Neonatal intestinal obstruction
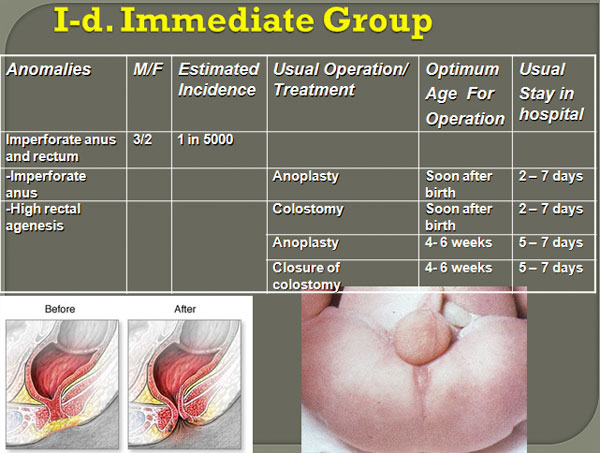
1- The immediate group
2- The intermediate group
3- The elective group
The immediate group
Conditions require immediate investigation and/or a definitive operation.
A particular important subgroup is neonatal emergencies.
Trauma, acute infections, abdominal emergencies acute scrotal conditions.
Neonatal emergencies
Most of these are the result of developmental abnormalities.
Developmental abnormalities causing:
Disorder of function.
Threaten life.
The best prognosis depends on:
Early diagnosis.
Speedy transport.
Effective surgical management.
Developmental anomalies
Affect the patients in three ways.
Anomalies causing obstructive, destructive and other consequences before birth.
Congenital diaphragmatic hernia.
Posterior urethral value.
Well-tolerated abnormalities without significant effect in utero.
Unruptured exomphalos.
Esophageal atresia.
Latent abnormalities.
Submucosal cleft palate.
Infection in urinary tract malformation.

دکتر سید محمد هادی امامی فر
lWhen
a neonate develops bilious vomiting, one should suspect a surgical condition
lAfter
a focused physical examination, a nasogastric or orogastric catheter should
be placed for gastric decompression to prevent further vomiting and
aspiration. This should be done before any diagnostic or therapeutic
maneuvers are performed.
lWhen
the patient is hemodynamically stabilized, appropriate imaging studies of
the abdomen should be performed. These would include plain abdominal films
and/or contrast studies
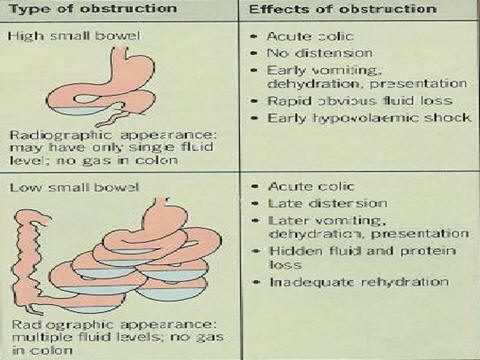
Intestinal obstruction with bilious vomiting in neonates can be
caused by
lduodenal
atresia,
lmalrotation
and volvulus,
l
jejunoileal atresia,
lmeconium
ileus,
land
necrotizing enterocolitis
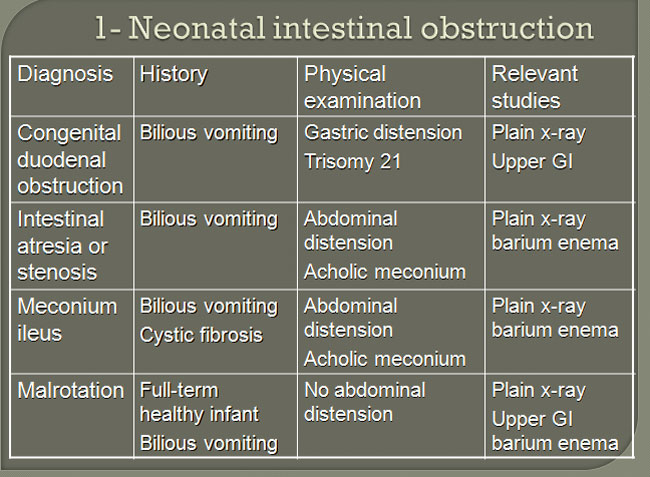
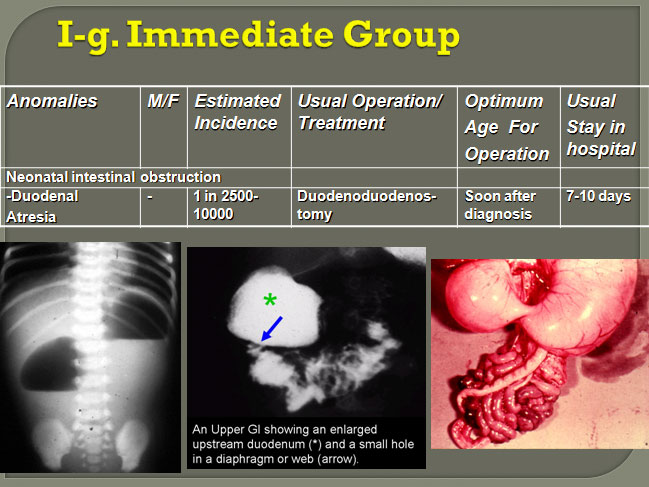
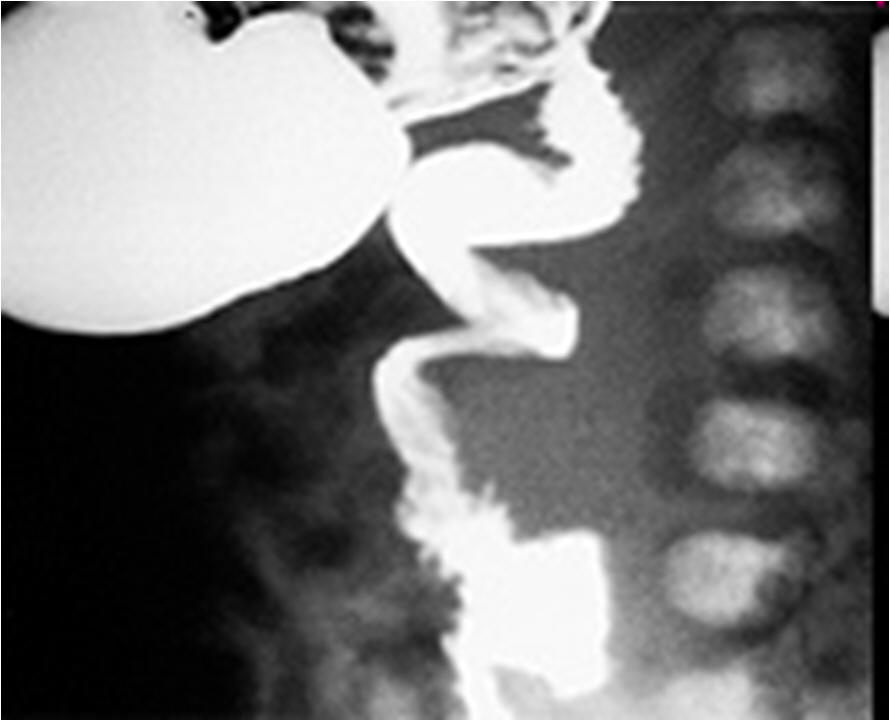
Duodenal atresia
lCause
and incidence
Embryogenic;
occurs in 1 per 5,000 live births; 25% have Down syndrome
lAge
of onset and presentation
Few hours after
birth; billious vomiting, no distention
lDiagnostic
procedure and findings
Abdominal film,
"double-bubble" sign
lPreoperative
management interval before surgery
Nasogastric
suction, IV fluids; 24 to 48 hours

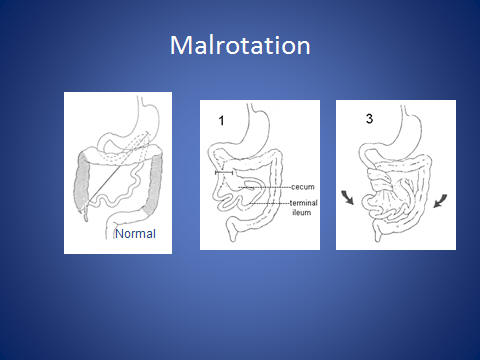
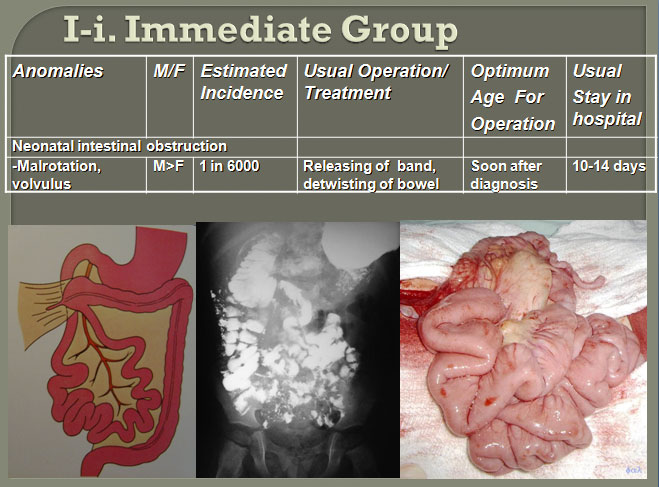
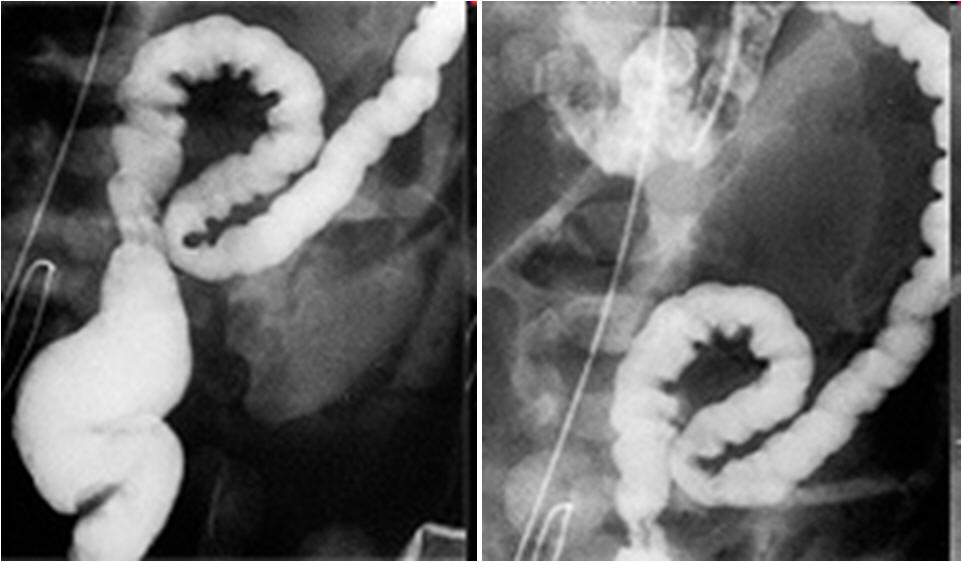
Malrotation with volvulus
lIncomplete
bowel rotation occurring during 7th to 12th weeks of gestation
lAt
3 to 7 days; bilious vomiting, rapid deterioration with volvulus
lUpper
GI spiral sign on ultrasound; abnormal location of the superior mesenteric
vessels
lNasogastric
suction, IV fluid; STAT surgery for symptomatic patients, within days for
others
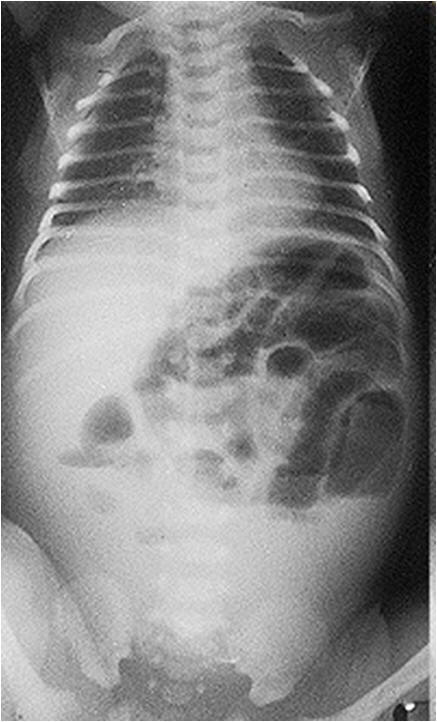
Jejunoileal atresia
lMesenteric
vascular accident during fetal life in 1 per 3,000 live births
lWithin
24 hours of birth; vomiting, abdominal distention
lAir-fluid
levels on abdominal film
lNasogastric
suction, IV fluids; 12 to 24 hours

Necrotizing ileus
lCause
unknown in 2.4 per 1,000 live births
l10
to 12 days after birth; distention, vomiting, bloody stools
lAbdominal
film; distention, pneumatosis, air in the aortal vein
lNasogastric
suction, IV fluids, nutrition, antibiotics for 10 days. When perforated,
immediate surgery
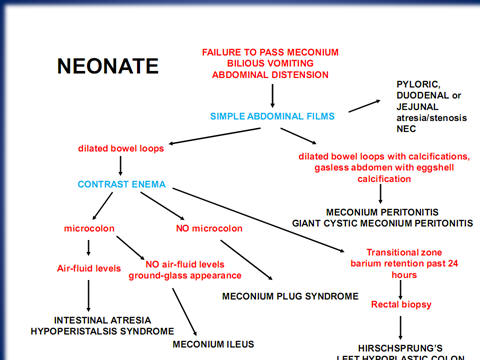
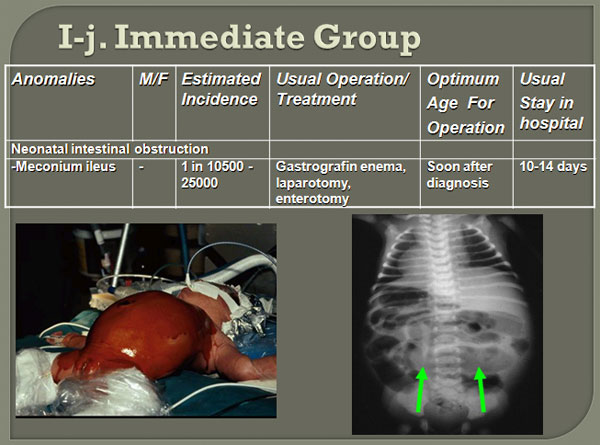
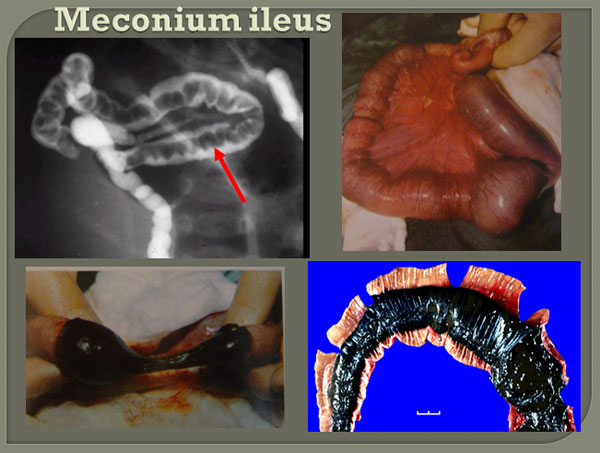
Meconium ileus
lGenetic,
occurs in 15% of newborns with cystic fibrosis, and in 1 per 5,000 to 10,000
live births
lImmediately
after birth; abdominal distention, bilious vomiting
lAbdominal
film; distention, air-fluid levels, sweat test, "ground-glass" sign
lMeconium
ileus is characterized by retention of thick tenacious meconium in the bowel
(ileum, jejunum or colon), which results in bowel obstruction.
lmucus
plugs may be evacuated after withdrawal of the examination finger.
lThe
plain abdominal films show distended loops of intestine with thickened bowel
walls.
l
A large amount of meconium mixed with swallowed air produces the so-called
"ground-glass" sign, which is typical of meconium ileu
lWhen
a Gastrografin enema is unsuccessful, laparotomy is indicated to evacuate
the obstructing meconium by enterotomy irrigation. Immediate surgery is
indicated in patients with complicated meconium ileus. Bowel resection for
perforation and/or obstruction related to kinking of the bowel is indicated,
usually requiring a temporary enterostomy.
دکتر محسن سنجری